
ALCOHOL:
The Drug We Pretend Isn’t a Drug

Every few months, usually after a teenager leaves my office to stare silently at their phone in the waiting room, a parent will quietly pull me aside.
“Can I ask you something?”
Of course.
“I know my son has probably had a few drinks with his friends. Maybe at a party. Maybe more than once. How worried should I be?”
The adults ask a version of the same question.
“Is it okay to have a glass of wine while taking my antidepressant?”
“What about beer with Vyvanse?”
“My psychiatrist before you said never. My primary care doctor said it was fine. Which is it?”
For years, my answer was simple: one or two drinks might be tolerated by many people, but beyond that, you are entering increasingly risky territory. I was trying to prevent the worst-case scenario. In retrospect, I was also engaging in a bit of wishful thinking. If I warned patients strongly enough, perhaps none of them would develop a drinking problem.
Medicine, unfortunately, does not work that way.
One of the strangest facts about alcohol is that we do not even talk about it as though it were a drug. We call it “having a drink,” “going out,” “happy hour,” or “unwinding.” Imagine saying, “I’m going home to enjoy a little neurotoxin before dinner.” The invitation list would shrink dramatically.
And yet alcohol is exactly that: a psychoactive substance that changes brain function, slows reaction time, impairs judgment, disrupts sleep, increases the risk of cancer, contributes to liver disease, raises blood pressure, and can produce life-threatening withdrawal when used heavily over time.¹˒²
It is also astonishingly common.
Roughly 70% of U.S. adults report drinking alcohol in the past year.³
Excessive alcohol use contributes to more than 175,000 deaths annually in the United States.⁴
Alcohol has been linked to more than 200 diseases and injury conditions recognized by major public health organizations.²
Nearly one-third of Americans will meet diagnostic criteria for an alcohol use disorder at some point during their lives.⁵
None of this means that everyone who enjoys a beer at a barbecue is headed for rehab. Far from it. One lesson psychiatry has taught me is that population statistics and individual patients are not the same thing. Some people can drink socially for decades without obvious consequences. Others lose jobs, marriages, health, or their lives.
That is precisely why I have become less interested in judging people and more interested in understanding them.
As journalist Kara Swisher has said, “Strong opinions, loosely held.” It is a useful reminder that good clinicians should be willing to update their beliefs when confronted with better evidence. That applies to politics, technology, and especially to alcohol.
Because if alcohol has one superpower besides intoxication, it is convincing perfectly intelligent people that they are the exception.
Can I Drink While Taking My Medication?
If I had a dollar for every patient who asked me, “Can I drink on this medication?”, I could probably retire and spend my afternoons judging clouds.
The honest answer, frustratingly, is it depends.
For years, I gave a fairly rigid response. One or two drinks might be acceptable, but anything beyond that was asking for trouble. I worried that if I sounded too permissive, someone would interpret “probably okay” as “go ahead and have six margaritas and text your ex.”
As my practice evolved, so did my thinking. I still encourage caution, but I have become much more interested in understanding who is asking the question. Is this someone who enjoys an occasional glass of champagne at a wedding? Or someone who regularly finishes a bottle of vodka while insisting they “hardly drink at all”? The same advice should not necessarily apply to both.
This is where medicine gets tricky. We study populations, but we treat individuals.
The good news is that many psychiatric medications do not produce catastrophic interactions with a single alcoholic drink. The bad news is that alcohol itself affects nearly every organ system and often magnifies medication side effects in ways that can be unpredictable.⁶
The biggest concern is not usually that the liver suddenly explodes. It is that judgment deteriorates, reaction times slow, blood pressure changes, balance worsens, and people make decisions they never would have made sober. I always think of a beer commercial that took place in an empty bar except for two male patrons. After an apparent swallow from his bottle, one turns to the other and says, “I love you, man.”
Some combinations deserve particular caution:
Notice one recurring theme: alcohol often acts as an amplifier.
That is especially true with benzodiazepines. I have heard patients casually describe taking “just a Xanax” before going out for drinks, as though combining two central nervous system depressants were no more consequential than pairing wine with cheese. In reality, the two substances can function as a force multiplier, each enhancing the other’s sedating effects and dramatically increasing the risks of falls, memory loss, impaired breathing, and overdose.⁸
Alcohol is involved in a substantial proportion of fatal motor vehicle crashes in the United States each year.⁹
Millions of Americans report combining alcohol with prescription medications that carry warnings about sedation or impaired coordination.¹⁰
Emergency departments routinely treat patients whose injuries stem less from the medication itself than from the medication-plus-alcohol combination.
The comedian Amy Poehler once joked, “Good for her, not for me.” I have always liked that phrase because it captures something medicine struggles with. Your neighbor may have two glasses of wine with dinner every Friday for thirty years and never encounter a serious problem. That does not mean the same choice is safe for you. The physician’s job is not to eliminate every pleasure from life. It is to help patients understand probabilities, recognize avoidable risks, and make informed decisions with eyes wide open.
And one final point that deserves repeating: if you have to ask whether mixing alcohol with a medication a good idea is, you are already demonstrating better judgment than many of the people who wind up in my stories.
When the Family Starts Doubting Itself
One of the saddest parts of my job is that the person with the drinking problem is often not the only one who ends up needing treatment. Sometimes it is the spouse.
Over the years, I have treated several patients whose husbands were almost certainly alcohol dependent. They did not come to see me because they drank. They came because they were anxious, depressed, couldn’t sleep, or had begun wondering if they were “going crazy.”
As I listened, a pattern emerged.
They would find empty bottles tucked behind boxes in the garage, under the driver’s seat of the car, or buried beneath yesterday’s recycling. They would notice slurred speech, the faint smell of alcohol disguised with mouthwash, or a personality change that appeared around 7:00 every evening with remarkable consistency. They had “conversations” about the drinking.
However, often they were told they were imagining things.
“You’re too sensitive.”
“I only had one.”
“You’re always looking for something to criticize.”
“Maybe if you weren’t so controlling, I wouldn’t have to hide it.”
After hearing enough versions of reality rewritten, many spouses begin to distrust their own senses. They replay conversations in their heads, second-guess their memories, and wonder whether they really are overreacting. Their confidence erodes, their self-esteem plummets, and they may apologize for asking perfectly reasonable questions.
That psychological maneuver has a name: gaslighting.¹⁶ It is not unique to alcohol use disorders, but addiction often creates fertile ground for it because preserving access to the substance becomes the overriding priority.
The deception itself can become astonishingly elaborate.
I’ve heard stories of bottles transferred into water containers, liquor purchased with cash to avoid credit card statements, recycling quietly discarded at gas stations, “business meetings” that seemed to occur with suspicious frequency at neighborhood bars, and staying late at the office because there was “so much work.”.
None of these behaviors necessarily prove addiction in isolation.
Taken together, however, they paint a picture that families know all too well.
Millions of Americans live with a family member who has an alcohol use disorder.¹⁷
Children raised in households affected by parental alcohol misuse are at increased risk for anxiety, depression, substance use disorders, and relationship difficulties later in life.¹⁸
Family members of people with addictions frequently report chronic stress, hypervigilance, sleep disturbance, and symptoms resembling trauma.¹⁹
One of the hardest lessons for partners to accept is that arguing with addiction rarely succeeds. Logic does not compete well against a substance that changes brain function. Evidence does not always penetrate denial.And promises made sincerely at 8:00 in the morning may evaporate by 8:00 that evening.
Comedian Amy Poehler once remarked, “There’s power in looking silly and not caring that you do.” Addiction often produces the opposite effect. People become so invested in maintaining the appearance that everything is fine that they expend enormous amounts of energy protecting the illusion instead of confronting the reality.
For the spouse, the emotional cost can be enormous. They begin by trying to save the relationship. Then they try to prevent embarrassment. Then they try to protect the children. Somewhere along the way, they stop asking, “Is my partner drinking too much?” and start asking, “What’s wrong with me?”
Usually, the answer is: not much. They’ve simply spent years trying to navigate a world in which the facts keep changing. One of the most healing moments in therapy can be surprisingly simple. A patient describes months or years of confusion, and I tell them, “Based on what you’ve shared with me, your reactions make sense.”
Sometimes validation is the first solid ground they’ve stood on in a very long time.
Looking at the Population Without Forgetting the Person
One of the most valuable techniques I learned during my training was motivational interviewing, a style of counseling that assumes people are more likely to change when they discover discrepancies in their own thinking than when someone lectures them.²⁰
That sounds obvious until you’ve actually tried arguing with addiction. Imagine a patient tells me, “Everybody does cocaine.”
I could respond, “No they don’t.”
That conversation would last about three seconds.
A better response might be, “Really? How many Americans do you think used cocaine in the past year?” Then we pull up the data together.
The answer is nowhere near “everybody.” In fact, the overwhelming majority of Americans did not use cocaine in the past year.²¹ The goal is not to embarrass the patient. The goal is to replace assumptions with evidence and let the patient draw their own conclusions.
The same thing happens with alcohol. Someone tells me, “Everybody gets drunk on weekends.”
Well...not exactly.
Someone else says, “Everyone drinks every night.”
Again, not really.
Our brains are terrible at estimating prevalence because we sample our own social circles. If all of your friends drink heavily, heavy drinking feels normal. If none of your friends drink, sobriety feels normal. Human beings mistake their immediate environment for the entire world.
Fewer than one in twenty Americans report using cocaine in the past year.²¹
Although alcohol use is common, a substantial minority of U.S. adults report not drinking at all in a given year.²²
National surveys consistently show that perceptions of peer substance use are often exaggerated, particularly among adolescents and young adults.²³
This is where my own thinking has changed over the years. Earlier in my career, I tended to think in terms of averages. If the average patient with a certain pattern of drinking had a poor outcome, I worried about everyone with that pattern. But patients are not averages.
Some people can have a nightly drink for years and stop one Tuesday because they’re training for a marathon. They experience no withdrawal, no cravings, and no urge to resume. Others begin drinking socially in college and, before they realize it, organize their entire lives around access to alcohol.
The statistics describe both groups. Neither statistic predicts which person is sitting across from me. This tension reflects a broader shift occurring throughout medicine. The old model relied heavily on population-based recommendations: what usually happens to most people. The newer approach attempts to combine those data with individual characteristics such as genetics, personality, psychiatric history, family history, trauma exposure, social supports, and life circumstances.
In other words, we still care about the forest. We just try not to lose sight of the tree.
Journalist Kara Swisher has built a career by questioning conventional wisdom and changing her mind when the evidence changes. Medicine should aspire to the same humility. Good clinicians should neither ignore the data nor become prisoners of it.
One patient may represent the rule. Another may represent the exception. Our job is to know the difference. That perspective has made me a better psychiatrist. It has also made me a little more skeptical whenever someone tells me that everyone drinks, everyone uses marijuana, everyone vapes, or everyone experiments with cocaine.
Usually, “everyone” turns out to mean “the five people I spent Saturday night with.”
The Generation That Chose Phones Over Parties
One of the more surprising developments in American public health over the past few decades is that many teenagers are drinking less, not more.²⁴
That often catches parents off guard.
Turn on the news, spend ten minutes on social media, or listen to adults complain about “kids these days,” and you might assume that Generation Z and the emerging Generation Alpha are awash in alcohol and drugs.
The data tell a more nuanced story.
Since the 1970s, national surveys have tracked substance use among American adolescents. The trend is remarkably consistent: alcohol use among high school students has fallen substantially, particularly since the late 1990s and early 2000s.²⁴˒²⁵
In the late 1970s, roughly three-quarters of high school seniors reported drinking alcohol within the previous year.²⁴
Today, that figure is closer to 40%, one of the lowest levels ever recorded.²⁴
Past-month alcohol use among 12th graders has dropped by more than half over the past several decades.²⁴
Binge drinking, once almost a rite of passage in many communities, has also declined dramatically among adolescents.²⁴
If you’re looking for a silver lining, this is one. But before we congratulate ourselves, another question arises.
If young people are drinking less, why do so many seem more anxious, lonely, and uncertain about the future?
That paradox fascinates me.
Many of my younger patients worry about issues that barely crossed my mind when I was their age. They wonder whether artificial intelligence will replace their careers before they begin. They question whether college debt will ever pay for itself. They worry about housing costs, climate change, political instability, and whether they will ever enjoy the kind of financial security their parents took for granted.
Some openly ask me, “What’s the point?”
Ironically, despite these enormous stressors, many are choosing not to self-medicate with alcohol in the way previous generations did. Why?
No one knows for certain, but several explanations have been proposed. Some experts believe today’s adolescents socialize less in person and more online, reducing opportunities for parties where alcohol is available. Others point to greater parental supervision, stricter enforcement of drunk driving laws, broader public awareness of substance-related harms, and changing cultural norms around wellness and fitness.²⁶
Then again, perhaps they have simply traded one dopamine source for another. A Friday night spent scrolling endlessly through videos is unlikely to produce a DUI, but it may not do much for emotional health either.
American teenagers spend many hours each day interacting with screens outside of school, with estimates often exceeding seven hours for entertainment alone.²⁷
Rates of adolescent alcohol use have generally fallen while concerns about depression, anxiety, loneliness, and self-harm have risen.²⁸
The relationship is almost certainly not causal in either direction, reminding us that multiple social forces can move simultaneously.
Comedian Amy Poehler once observed, “No matter what, keep finding new roads to travel.” I sometimes think our patients do exactly that. Humans are remarkably creative at finding ways to regulate emotion. One generation sneaks beer into the woods behind the football field. Another spends six hours on TikTok until two in the morning.
The coping strategy changes. The underlying need often does not. As psychiatrists, parents, and teachers, our challenge is not merely to prevent substance use. It is to help young people build lives in which they need fewer escapes in the first place.
And that may be harder than confiscating a six-pack.
If Aliens Landed Tomorrow, They’d Probably Ban Alcohol First
Imagine a group of scientists from another planet arrives on Earth.
They discover a clear liquid that impairs judgment, slows reaction time, increases aggression in some users, damages the liver, raises the risk of several cancers, disrupts sleep, contributes to cardiovascular disease, can produce fatal withdrawal, kills tens of thousands of people in motor vehicle crashes worldwide, and is implicated in countless assaults, suicides, and broken families.
Then they learn that humans sell this substance in grocery stores. They would think we’ve lost our minds. One of the enduring oddities of modern life is that we classify drugs more by history and culture than by pharmacology. Alcohol is legal, so we tend to think of it as relatively benign. Heroin is illegal, so we instinctively assume it must be far worse in every respect.
Reality is more complicated.
Researchers who study drug policy often distinguish between harm to the individual user and harm to society as a whole. A substance can be devastating for the person taking it while affecting relatively few other people simply because it is uncommon. Another can create enormous public health damage because millions of people consume it every weekend.²⁹
That helps explain why alcohol routinely ranks among the most harmful psychoactive substances when broader social consequences are included.
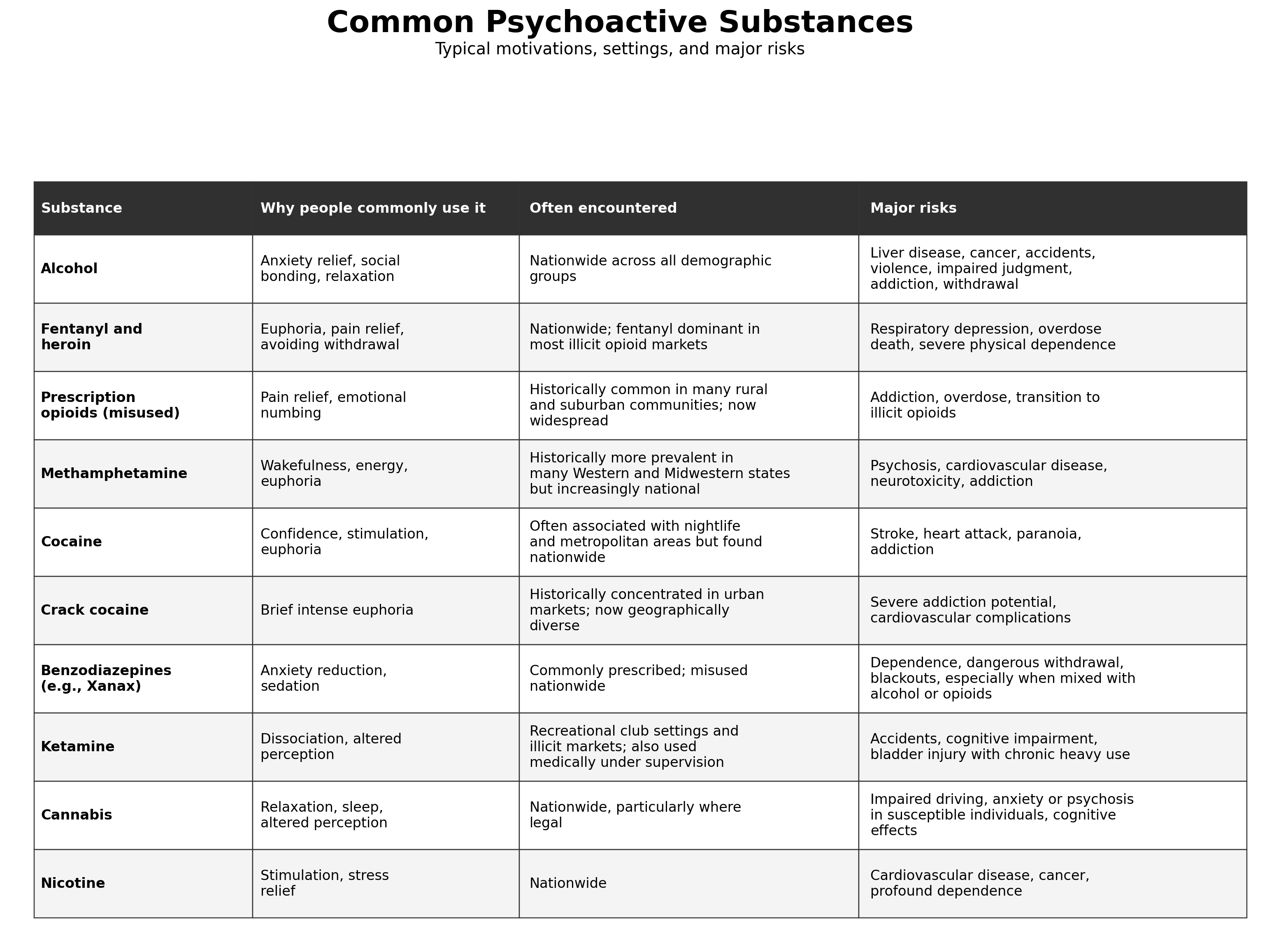
*Patterns change over time and should be interpreted as broad epidemiologic observations rather than rigid geographic rules.
Now notice something curious. The table says almost nothing about how many people use these substances. That matters enormously.
If one million people use a dangerous drug and seventy million use another somewhat less dangerous one, the second drug may produce vastly greater societal harm simply because of the number of people exposed.
Alcohol is the perfect example.
Alcohol contributes to an estimated 178,000 deaths annually in the United States.³⁰
More than 2 billion people worldwide consume alcohol.³¹
Excessive alcohol use costs the U.S. economy hundreds of billions of dollars each year through lost productivity, health care expenditures, and criminal justice involvement.³²
Then there are combinations.
If I could wave a magic wand and eliminate one pairing from emergency departments across America, it might be benzodiazepines and alcohol.
Patients often underestimate this mixture because each substance is legal when prescribed or purchased appropriately. Together, however, they amplify one another’s effects. Memory disappears. Judgment evaporates. Falls become more likely. Breathing slows. Fatal overdoses become possible.³³
The same is true for alcohol and opioids. Individually, each suppresses the central nervous system. Combined, they can suppress it enough that a person simply stops breathing.
Comedian Nikki Glaser has joked that alcohol convinced her she was having fun even when she wasn’t. That observation captures something profound. Psychoactive substances don’t merely change behavior. They change our perception of behavior. The person becoming progressively impaired is often the least reliable judge of how impaired they actually are.
Which brings me back to my office. When patients ask whether alcohol is “safe,” I increasingly think they’re asking the wrong question.
The better question is:
Safe for whom? Safe at what dose? Safe with which medications? Safe with what family history? Safe under what circumstances?
Medicine rarely deals in absolutes.
But if there is one lesson the data teach again and again, it is that the most dangerous drug is not necessarily the one that is illegal. Sometimes it’s the one waiting in the refrigerator.
The Most Important Question Isn’t “How Much Do You Drink?”
When I first started practicing psychiatry, I thought the most important question I could ask about alcohol was, “How much do you drink?” It seemed straightforward enough. Count the number of drinks, compare it with established guidelines, and decide whether there was a problem. Years later, I still ask about quantity, but I have become far more interested in the story behind the number. I want to know what alcohol actually does for the person sitting across from me. Does it quiet their anxiety? Help them fall asleep? Make social situations bearable? Ease loneliness after a divorce. The answer to those questions often tells me much more than a tally on a calendar ever could.³⁴
That shift in perspective came, in part, from learning motivational interviewing. The philosophy behind it is deceptively simple: people are more likely to change when they discover the inconsistencies in their own thinking than when someone points them out with a wagging finger. If I spend an hour insisting that a patient drinks too much, they may spend the next hour mentally constructing arguments about why I am wrong. If, instead, I ask what alcohol gives them, what it costs them, and what life might look like without it, they often begin to answer questions they did not realize they had been avoiding.
The pattern I hear over and over again is surprisingly consistent. Very few people begin drinking with the goal of becoming addicted. They drink because, at least initially, alcohol solves a problem. It takes the edge off after a difficult day. It quiets the internal critic at a party. It softens grief, numbs disappointment, or provides a fleeting sense of confidence. For a while, the arrangement seems almost magical.
Then something subtle changes. The drink that was once reserved for celebrations becomes part of an ordinary evening. The ordinary evening becomes every evening. Eventually, the person is no longer drinking because alcohol makes them feel good. They are drinking because without it they feel distinctly worse. The brain, having learned that relief is only a glass away, begins demanding the solution it was taught to expect.
By the time family members notice this transition, the consequences often extend far beyond the bottle itself. Relationships become strained by broken promises and half-truths. Partners find themselves questioning conversations they clearly remember. Children learn to gauge the atmosphere in the house by the sound of footsteps or the smell on someone’s breath. The addiction slowly expands until it occupies emotional space in everyone around it, not just the person consuming the alcohol.
The statistics reflect this reality. Many people with alcohol use disorder do not recognize the severity of their condition until significant personal or medical consequences have accumulated.³⁵ Family members frequently seek treatment for anxiety, depression, insomnia, or chronic stress generated by a loved one’s substance use rather than for problems of their own making.¹⁹ Research also suggests that earlier intervention generally produces better outcomes than waiting for someone to hit a dramatic “rock bottom,” despite how deeply that myth remains embedded in popular culture.³⁶
One of the biggest lessons I have learned over the years is that public health and individual patient care are not competing philosophies but complementary ones. The epidemiologist in me wants to understand what happens across entire populations, looking for patterns that can inform prevention and policy. The psychiatrist in me knows that none of those averages perfectly describes the person sitting in my office. Population statistics tell us what is likely to happen. Clinical medicine is about discovering what is happening to this particular human being.
That distinction has made me both more cautious and more compassionate. I have seen patients who decided one day to stop drinking and simply did so, experiencing little difficulty beyond changing an old habit. I have seen others fight cravings for years despite every sincere effort, requiring medication, psychotherapy, support groups, and repeated attempts before achieving lasting sobriety. The existence of one group does not invalidate the experience of the other. Human beings are wonderfully, frustratingly variable.
Journalist Kara Swisher has often emphasized the importance of revising one’s views when confronted with better evidence. I think medicine demands the same intellectual humility. The more years I spend practicing, the less interested I become in rigid rules and the more interested I become in understanding context, motivation, resilience, and vulnerability. Good care requires all of them.
So when a parent quietly asks whether they should worry that their teenager had a couple of drinks at a party, my mind no longer goes immediately to the alcohol. Instead, I wonder about the teenager’s life as a whole. Do they have friends they trust? Can they tolerate disappointment? Are they overwhelmed by anxiety or depression? Do they have reasons to feel hopeful about adulthood? Are they experimenting because they are curious, because they are lonely, or because they have already discovered that alcohol temporarily fixes something they cannot otherwise explain?
Over time, I have come to believe that substances are rarely the original problem. More often, they are the first solution the brain stumbles upon. The real challenge for psychiatry is not simply persuading someone to put down the bottle. It is helping them build a life with enough purpose, connection, and healthier coping strategies that the bottle gradually loses its appeal. When that happens, abstinence is no longer an act of constant willpower. It becomes the natural consequence of no longer needing alcohol to stay afloat.
If you enjoyed this article, found it helpful, or know someone whose family has been touched by alcohol or addiction, please consider liking, commenting, sharing, and subscribing. Those simple actions help these essays reach readers who might never otherwise see them.
If you’d like to support my work and help keep these long-form articles coming, please consider upgrading to a paid subscription. And if you’re ever in Boulder, stop by and say hello. There might even be cookies waiting for you.
For more writing on psychiatry, neuroscience, ADHD, autism, sleep, and the strange ways our brains navigate modern life, visit Boulder Psychiatry Associates and follow along here on Substack.
Notes and Sources
National Institute on Alcohol Abuse and Alcoholism (NIAAA). Alcohol’s Effects on Health and Alcohol-Medication Interactions: Potentially Dangerous Mixes. Bethesda, MD: National Institutes of Health.
World Health Organization (WHO). Global Status Report on Alcohol and Health. Geneva: World Health Organization.
Substance Abuse and Mental Health Services Administration (SAMHSA). National Survey on Drug Use and Health (NSDUH): Detailed Tables. Rockville, MD: U.S. Department of Health and Human Services.
Centers for Disease Control and Prevention (CDC). Alcohol and Public Health and Alcohol-Related Disease Impact (ARDI). Atlanta, GA: CDC.
Grant BF, Chou SP, Saha TD, et al. “Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV Alcohol Use Disorder in the United States.” JAMA Psychiatry. Related findings from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC).
National Highway Traffic Safety Administration (NHTSA). Traffic Safety Facts: Alcohol-Impaired Driving. Washington, DC: U.S. Department of Transportation.
U.S. Food and Drug Administration (FDA). Prescribing information and boxed warnings regarding benzodiazepines, opioids, and alcohol-related central nervous system depression.
National Institute on Drug Abuse (NIDA). Drugs, Brains, and Behavior: The Science of Addiction. Bethesda, MD: National Institutes of Health.
Koob GF, Volkow ND. “Neurobiology of Addiction: A Neurocircuitry Analysis.” The Lancet Psychiatry.
Roehrs T, Roth T. “Sleep, Sleepiness, Sleep Disorders, and Alcohol Use and Abuse.” Sleep Medicine Reviews.
Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. New York: Guilford Press.
Stern R. The Gaslight Effect. New York: Harmony Books.
Orford J, Copello A, Velleman R, Templeton L. Research on the impact of addiction on spouses and family members, including stress, psychological burden, and family functioning.
Anda RF, Felitti VJ, et al. Adverse Childhood Experiences (ACE) studies and subsequent literature on parental substance use and long-term mental health outcomes.
Monitoring the Future Study. Johnston LD, Miech RA, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Annual reports on adolescent alcohol and drug use. Ann Arbor, MI: Institute for Social Research, University of Michigan.
Common Sense Media. Research reports on adolescent screen use and digital media consumption.
Perkins HW. Research on normative misperceptions and perceived peer substance use among adolescents and young adults.
Nutt DJ, King LA, Phillips LD. “Drug Harms in the UK: A Multicriteria Decision Analysis.” The Lancet. A landmark comparison of the relative harms of alcohol and other psychoactive substances to individuals and society.
Kelly JF, Humphreys K, Ferri M. Research on recovery outcomes and the benefits of early intervention in substance use disorders.